
CPR Study guide 2021
Online CPR Cheat sheet
cpr study guide, cpr cheat sheet, cpr reference, American Heart cpr cheat sheet. free cpr study guide , American Heart CPR Training guide, Steps to do CPR , how to do american heart cpr , cpr bls cheatsheet
cpr cheat sheet, cpr cheat sheet online, cpr cheat sheet 2021, cpr cheat sheet american heart association, cpr cheat sheet red cross, infant cpr cheat sheet, first aid cpr cheat sheet, child cpr cheat sheet, pediatric, cpr cheat sheet. bls cpr cheat sheet
learn CPR, CPR study guide, CPR for beiginers, CPR crash course, cpr exam prep, online cpr certification for healthcare providers, online cpr certification canada, online cpr certification aha, online cpr certification free, online cpr certification for healthcare providers american heart association, online cpr certification renewal, online cpr certification, online cpr certification california, online cpr certification florida, free online cpr certification, free online cpr certification red cross, best online cpr certification, is online cpr certification legitimate, is online cpr certification valid, cheap online cpr certification, osha online cpr certification, online bls cpr certification, online first aid and cpr certification, online first aid and cpr certification, american heart association, online american red cross cpr certification, online aed cpr certification, online osha cpr certification
cpr answer, key american red cross, online cpr cheat sheet, online review questions, bls study guide, quizlet bls provider manual, 2019 pdf free first aid. cheat sheetcpr study guide quizlet aha bls, reference cardinfant bls surgery centervinay guda bls simulation answersbls exam questions and answers 2019 pdfaha cpr fact sheet2015 bls study guidecpr practice test 20192020 cpr guidelinesprocpr loginprofirstaid loginprotraining videoscpr first aidbls provider manual ebook freepals written exam 50 questionsamerican red cross cpr test answer key 2019american heart association cpr test quizletbasic life support provider manual (italian)how to pass cpr skills test cpr and first aid study guide quizletcpr book pdfcpr test center reviews
Cardiopulmonary resuscitation (CPR) is an emergency procedure that can help save a person's life if their breathing or heart stops. When a person's heart stops beating, they are in cardiac arrest. ... CPR uses chest compressions to mimic how the heart pumps. These compressions help keep blood flowing throughout the body.
Cardiopulmonary resuscitation (CPR) is an emergency procedure that combines chest compressions often with artificial ventilation in an effort to manually preserve intact brain function until further measures are taken to restore spontaneous blood circulation and breathing in a person who is in cardiac arrest. It is recommended in those who are unresponsive with no breathing or abnormal breathing, for example, agonal respirations.
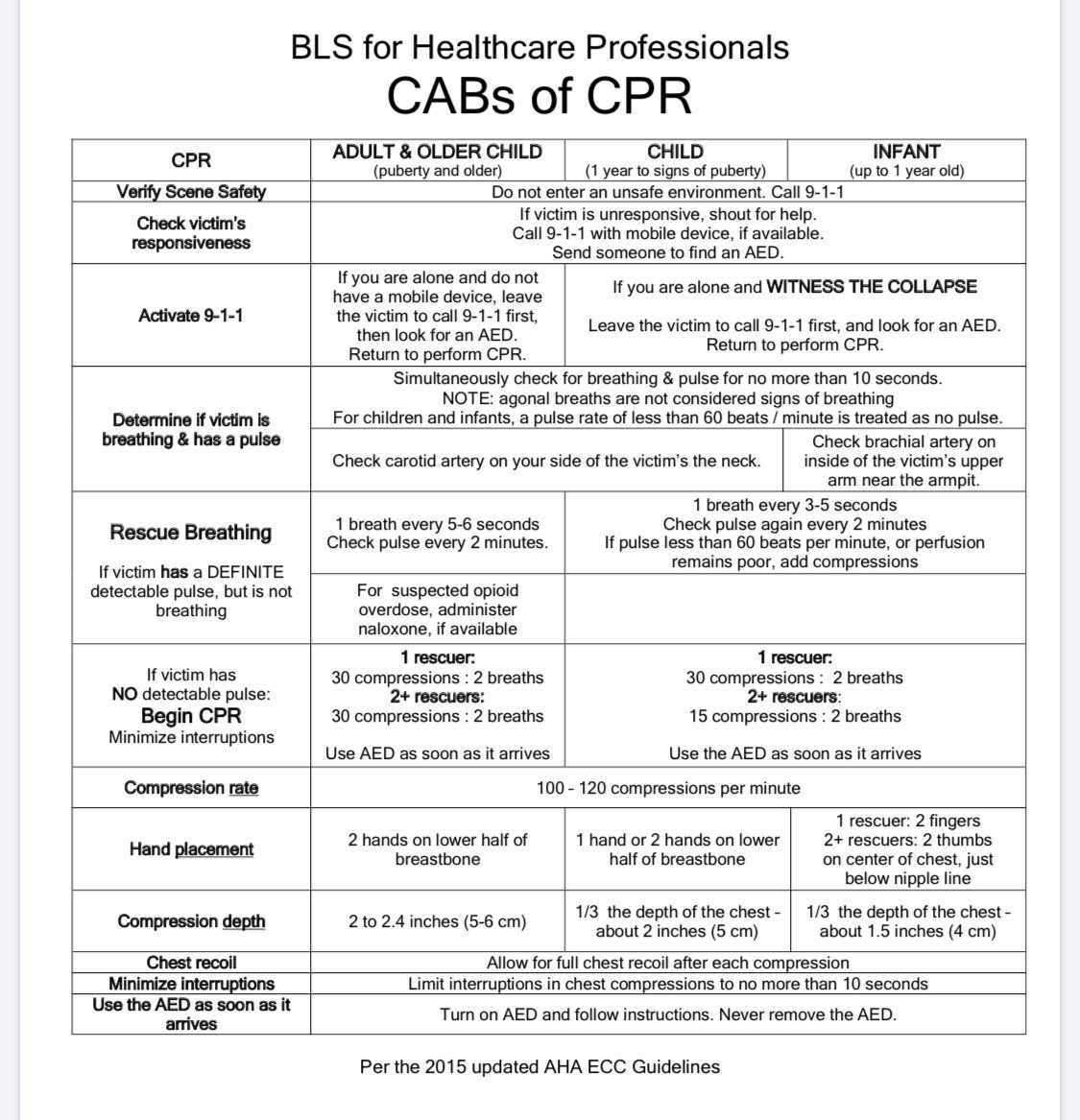
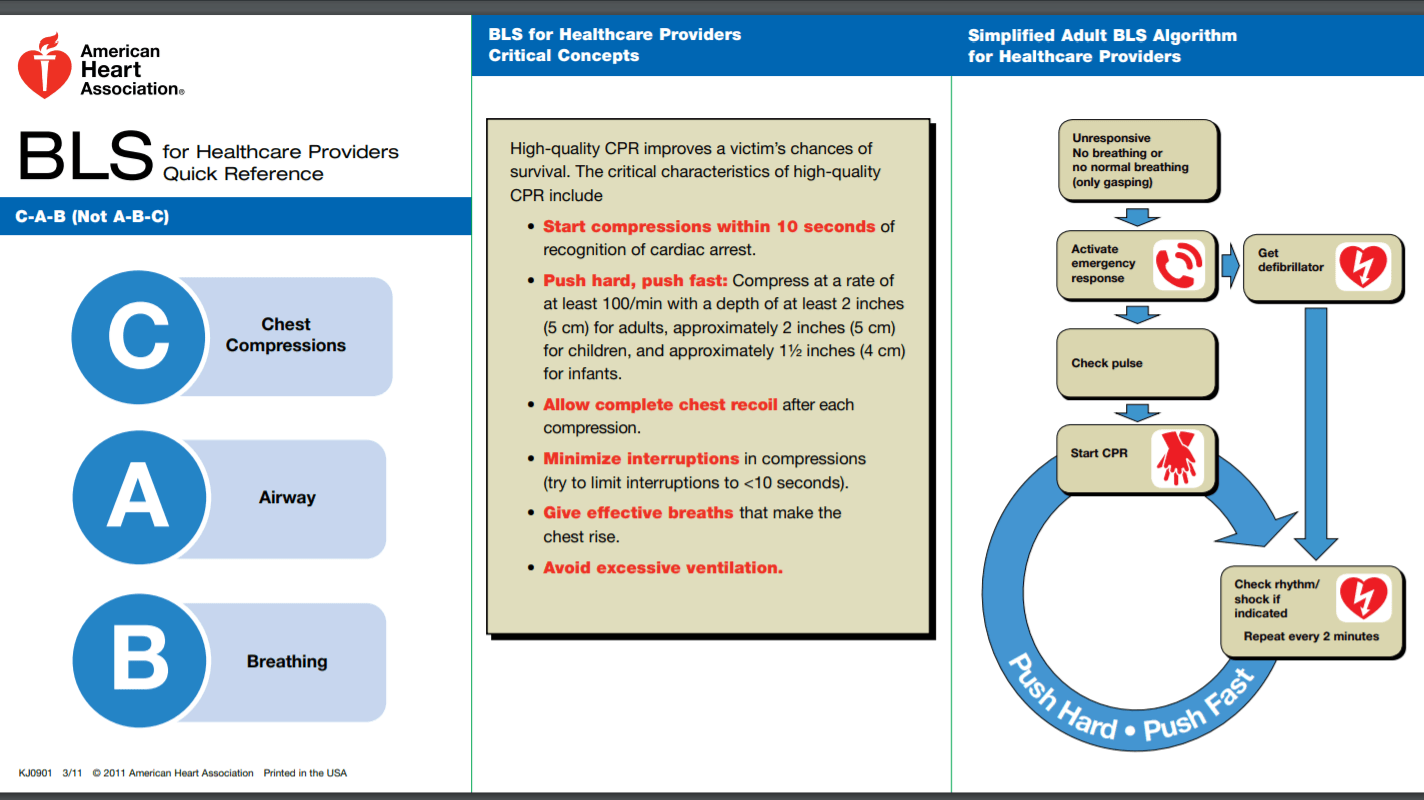
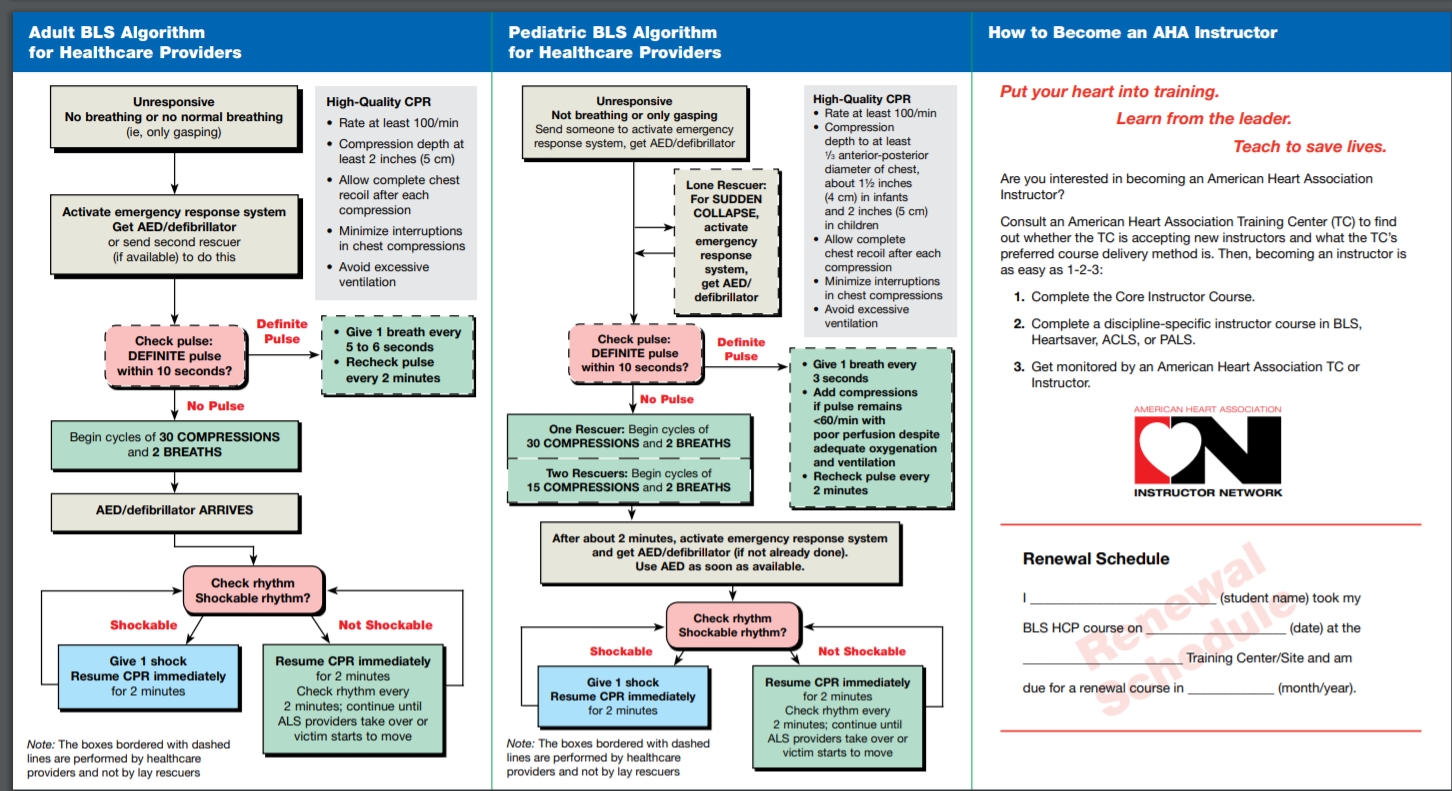
CPR involves chest compressions for adults between 5 cm (2.0 in) and 6 cm (2.4 in) deep and at a rate of at least 100 to 120 per minute. The rescuer may also provide artificial ventilation by either exhaling air into the subject's mouth or nose (mouth-to-mouth resuscitation) or using a device that pushes air into the subject's lungs (mechanical ventilation). Current recommendations place emphasis on early and high-quality chest compressions over artificial ventilation; a simplified CPR method involving chest compressions, is only recommended for untrained rescuers. In children, however, only doing compressions may result in worse outcomes because, in children, the problem normally arises from a respiratory, rather than cardiac, problem.[1] Chest compression to breathing ratios is set at 30 to 2 in adults.
CPR alone is unlikely to restart the heart. Its main purpose is to restore partial flow of oxygenated blood to the brain and heart. The objective is to delay tissue death and to extend the brief window of opportunity for a successful resuscitation without permanent brain damage. Administration of an electric shock to the subject's heart, termed defibrillation, is usually needed in order to restore a viable, or "perfusing", heart rhythm. Defibrillation is effective only for certain heart rhythms, namely ventricular fibrillation or pulseless ventricular tachycardia, rather than asystole or pulseless electrical activity. Early shock, when appropriate, is recommended. CPR may succeed in inducing a heart rhythm that may be shockable. In general, CPR is continued until the person has a return of spontaneous circulation (ROSC) or is declared dead.
Medical uses
Chest compressions at 100 - 120 per minute on a dummy.
CPR is indicated for any person unresponsive with no breathing or breathing only in occasional agonal gasps, as it is most likely that they are in cardiac arrest. If a person still has a pulse but is not breathing (respiratory arrest) artificial ventilations may be more appropriate, but, due to the difficulty people have in accurately assessing the presence or absence of a pulse, CPR guidelines recommend that lay persons should not be instructed to check the pulse, while giving healthcare professionals the option to check a pulse. In those with cardiac arrest due to trauma, CPR is considered futile but still recommended. Correcting the underlying cause such as a tension pneumothorax or pericardial tamponade may help.
Effectiveness
CPR oxygenates the body and brain for defibrillation and advanced life support. Even in the case of a "non-shockable" rhythm, such as pulseless electrical activity (PEA) where defibrillation is not indicated, effective CPR is no less important. Used alone, CPR will result in few complete recoveries, though the outcome without CPR is almost uniformly fatal.
Studies have shown that immediate CPR followed by defibrillation within 3–5 minutes of sudden VF cardiac arrest dramatically improves survival. In cities such as Seattle where CPR training is widespread and defibrillation by EMS personnel follows quickly, the survival rate is about 20 percent for all causes and as high as 57 percent if a witnessed "shockable" arrest. In cities such as New York, without those advantages, the survival rate is only 5 percent for witnessed shockable arrest.
Similarly in-hospital CPR is more successful when arrests are witnessed or are in the ICU or in patients wearing heart monitors, where the arrests are noticed immediately.
Compression-only CPR may be less effective in children than in adults, as cardiac arrest in children is more likely to have a non-cardiac cause. In a 2010 prospective study of cardiac arrest in children (age 1–17) for arrests with a non-cardiac cause, provision by bystanders of conventional CPR with rescue breathing yielded a favorable neurological outcome at one month more often than did compression-only CPR . For arrests with a cardiac cause in this cohort, there was no difference between the two techniques . This is consistent with American Heart Association guidelines for parents.
When done by trained responders, 30 compressions interrupted by two breaths appears to have a slightly better result than continuous chest compressions with breaths being delivered while compressions are ongoing.
There is a higher proportion of patients who achieve spontaneous circulation (ROSC), where their heart starts beating on its own again, than ultimately survive to be discharged from hospital (see table above).
Measurement of end-tidal carbon dioxide during CPR reflects cardiac output and can predict chances of ROSC.
59% of CPR survivors lived over a year; 44% lived over 3 years, based on a study of CPR done in 2000–2008.
Consequences.
Performing CPR is advised as a last resort intervention, for when a person is not breathing and therefore would certainly die without it.
Survival rates: In US hospitals in 2017, 26% of patients who received CPR survived to hospital discharge. In 2017 in the US, outside hospitals, 16% of people whose cardiac arrest was witnessed survived to hospital discharge.
Since 2003, widespread cooling of patients after CPR and other improvements have raised survival and reduced mental disabilities.
Organ donation.
Organ donation is usually made possible by CPR, even if CPR does not save the patient. If there is a Return of spontaneous circulation (ROSC), all organs can be considered for donation. If the patient does not achieve ROSC, and CPR continues until an operating room is available, the kidneys and liver can still be considered for donation. 1,000 organs per year in the US are transplanted from patients who had CPR. Donations can be taken from 40% of patients who have ROSC and later become brain dead. Up to 8 organs can be taken from each donor, and an average of 3 organs are taken from each patient who donates organs.
Mental abilities.
Mental abilities are about the same for survivors before and after CPR for 89% of patients, based on before and after counts of 12,500 US patients' Cerebral-Performance Category ( codes in a 2000-2009 study of CPR in hospitals. 1% more survivors were in comas than before CPR. 5% more needed help with daily activities. 5% more had moderate mental problems and could still be independent.
For CPR outside hospitals, a Copenhagen study of 2,504 patients in 2007-2011 found 21% of survivors developed moderate mental problems but could still be independent, and 11% of survivors developed severe mental problems, so they needed daily help. Two patients out of 2,504 went into comas (0.1% of patients, or 2 out of 419 survivors, 0.5%), and the study did not track how long the comas lasted.
Most people in comas start to recover in 2–3 weeks. 2018 guidelines on disorders of consciousness say it is no longer appropriate to use the term "permanent vegetative state." Mental abilities can continue to improve in the six months after discharge, and in subsequent years. For long-term problems, brains form new paths to replace damaged areas.
Injuries
Injuries from CPR vary. 87% of patients are not injured by CPR Overall, injuries are caused in 13% (2009-12 data) of patients, including broken sternum or ribs (9%), lung injuries (3%), and internal bleeding (3%). The internal injuries counted here can include heart contusion, hemopericardium, upper airway complications, damage to the abdominal viscera − lacerations of the liver and spleen, fat emboli, complications − pneumothorax, hemothorax, lung contusions. Most injuries did not affect care; only 1% of those given CPR received life-threatening injuries from it.
Broken ribs are present in 3%[ of those who survive to hospital discharge, and 15% of those who die in the hospital, for an average rate of 9% (2009-12 data) to 8% (1997–99). In the 2009-12 study, 20% of survivors were older than 75.A study in the 1990s found 55% of CPR patients who died before discharge had broken ribs, and a study in the 1960s found 97% did; training and experience levels have improved. Lung injuries were caused in 3% of patients and other internal bleeding in 3% (2009–12).
Bones heal in 1–2 months. Training and experience levels have improved since the study in the 1990s which found 55% broken ribs among CPR patients who died before discharge, and the study in the 1960s which found 97%.
The costal cartilage also breaks in an unknown number of additional cases, which can sound like breaking bones.
The type and frequency of injury can be affected by factors such as sex and age. A 1999 Austrian study of CPR on cadavers, using a machine which alternately compressed the chest then pulled it outward, found a higher rate of sternal fractures in female cadavers (9 of 17) than male (2 of 20), and found the risk of rib fractures rose with age, though they did not say how much.Children and infants have a low risk of rib fractures during CPR, with an incidence less than 2%, although, when they do occur, they are usually anterior and multiple.
Where CPR is performed in error by a bystander, on a person not in cardiac arrest, around 2% have injury as a result (although 12% experienced discomfort).
A 2004 overview said, "Chest injury is a price worth paying to achieve optimal efficacy of chest compressions. Cautious or faint-hearted chest compression may save bones in the individual case but not the patient’s life."